Why HMG and Clomid Should Not Be Used Together
Understanding the Endocrine Conflict in HPTA Recovery
Hormonal recovery is not about stacking more compounds.
It is about understanding physiology.
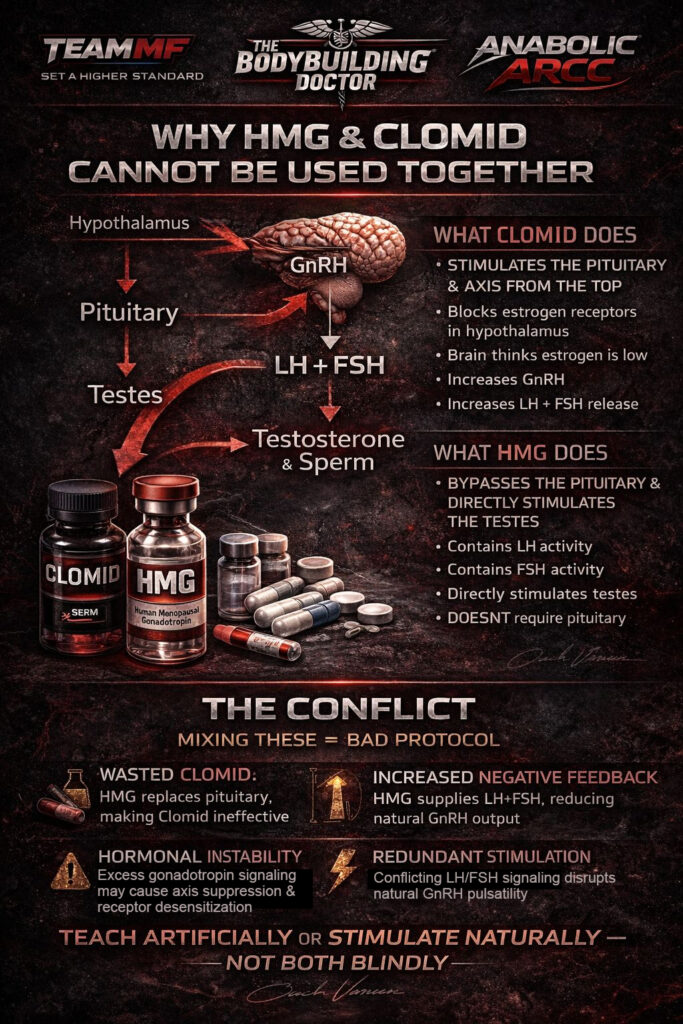
One of the most common mistakes seen in post-cycle therapy and fertility protocols is the blind combination of HMG (Human Menopausal Gonadotropin) with Clomiphene Citrate (Clomid).
At first glance, both seem beneficial.
Both increase LH and FSH activity.
But the mechanism matters.
Understanding the HPTA Axis
The Hypothalamic–Pituitary–Testicular Axis (HPTA) functions as follows:
Hypothalamus
↓
GnRH (Gonadotropin Releasing Hormone)
↓
Pituitary
↓
LH + FSH
↓
Testes
↓
Testosterone & Spermatogenesis
Recovery must respect this hierarchy.
What Clomid Does
Clomid is a Selective Estrogen Receptor Modulator (SERM).
Mechanism:
- Blocks estrogen receptors at the hypothalamus
- Brain perceives low estrogen
- GnRH secretion increases
- Pituitary releases more LH & FSH
- Testes are stimulated naturally
Clomid works at the top of the axis.
It stimulates the brain and pituitary to resume function.
This requires a functional pituitary gland.
What HMG Does
HMG contains both LH and FSH activity.
Mechanism:
- Directly stimulates the testes
- Bypasses the pituitary
- Does not rely on GnRH signaling
HMG works at the bottom of the axis.
It replaces the pituitary output artificially.
The Core Conflict
Using Clomid and HMG simultaneously creates redundancy.
Clomid attempts to increase endogenous LH/FSH production.
HMG supplies LH/FSH externally.
When exogenous gonadotropins are introduced:
- Downstream testosterone rises
- Negative feedback increases
- GnRH pulsatility may reduce
- Pituitary output can decrease
This reduces the necessity of Clomid’s action.
In simple terms:
You are trying to stimulate LH/FSH production
while simultaneously injecting LH/FSH.
This can create:
- Redundant stimulation
- Hormonal instability
- Inconsistent feedback signaling
- Potential receptor desensitization
Why Sequential Use Is Superior
Structured fertility or recovery protocols may use:
Phase 1:
HCG ± HMG
(Restoration of intratesticular function and spermatogenesis)
Phase 2:
Transition to Clomid
(Reactivation of pituitary-driven endogenous control)
This approach respects physiology.
Stacking them aggressively without monitoring does not.
When Might Combination Be Considered?
In rare, medically supervised cases such as:
- Severe hypogonadotropic hypogonadism
- Long-term suppression with pituitary inactivity
- Fertility specialist-guided protocols
Even then, dosing must be precise and monitored with bloodwork.
This is not general bodybuilding PCT logic.
The Professional Rule
Either:
Stimulate the axis from the brain
OR
Replace gonadotropin signaling temporarily
Do not confuse the endocrine system with blind stacking.
Hormonal recovery requires structured planning, not panic dosing.
For Structured HPTA Recovery & Fertility Guidance
Consult Team Muscle Factory
The Bodybuilding Doctor
Anabolic Arcc
Scientific recovery. Structured protocols. Real endocrinology.

